Each month we compile a short-list of recently-published papers (full list here) in the world of running science and break them into bite-sized chunks so you can digest them as food for thought to help optimise your training. To help wash it all down, we even review our favourite beers of the month.
Welcome to this month's installment of our "Nerd Alert". We hope you enjoy it.
Share this nerd alert:
Click the title of each article to "drop-down" the summary.
What was the hypothesis or research question?
Running has a high sports injury rate and there additional sex-related risk factors for certain injuries but a systematic review does not exist. Therefore, the authors systematically investigated the differences in injury rates between female and male runners.
What did they do to test the hypothesis or answer the research question?
— Prospective studies reporting running related injury rates for both sexes were included in the systematic review, conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
— A random-effects meta-analysis was used to pool the risk ratios (RR) for the occurrence of injuries in female vs. male runners.
— After their literature search in PubMed, Web of Science, PEDro, and SPORTDiscus databases, 38 studies were included, covering 35,689 participants, and the odds ratios of 31 studies were pooled in the meta-analysis.
What did they find?
— There were 21 injuries per 100 female runners (
95% confidence intervalthe estimated range of values within which there is a 95% probability that the true value is contained.
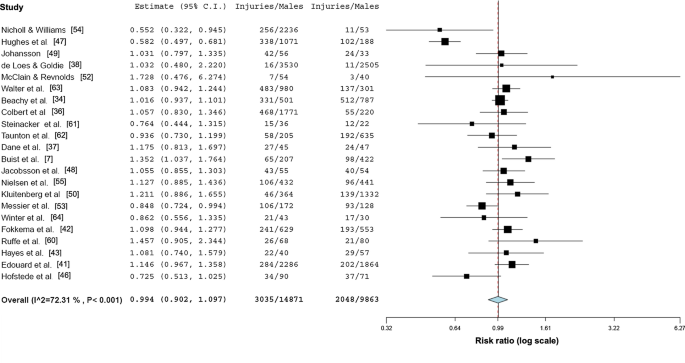
[CI] 19.9–21.7) and 20 injuries per 100 male runners (95% CI 19.7–21.1). These total injury rates were not different between female and male runners (
relative riskthe ratio of the probability of an outcome in the treatment group to the probability of an outcome in the control group. If RR = 1 this means that treatment does not affect the outcome (i.e. no differences between groups). RR less than 1 means that the risk of the outcome is decreased by the treatment, which is therefore protective. RR greater than 1 means that the risk of the outcome is increased by the treatment.
= 0.99, 95% CI 0.90–1.10). Since the relative risk is very close to 1 and since the 95% CI overlaps 1, the risk of injury is not different between groups.
Forest plot depicting the meta-analytical results comparing risk ratios for male and female runners regarding injuries per 100 runners
Despite there not being any sex differences in total injury rates, there were some notable differences in specific injuries:
— Shorter competition distances (10 km or less) increased total injury risk in female runners: relative risk (compared to longer than 10 km) = 1.08 (95% CI 1.00–1.69), i.e. an 8% higher risk.
— Female runners had more bone stress injuries than male runners: the relative risk for males (compared to females) = 0.52 (95% CI 0.36–0.76), i.e. an bone stress injury occurs about half as often in men.
Forest plot depicting the meta-analytical results comparing risk ratios for male and female runners regarding bone stress injuries.
— Male runners had more Achilles tendon injuries than female runners: the relative risk for males (compared to females) = 1.86 (95% CI 1.25–2.79), i.e. an Achilles tendon injury occurs nearly twice as often in men.
Forest plot depicting the meta-analytical results comparing risk ratios for male and female runners regarding Achilles tendinopathy.
What were the strengths?
— The systematic review protocol was published so it is easy in future to add new studies as and when they become available.
— Three independent authors extracted data from the studies.
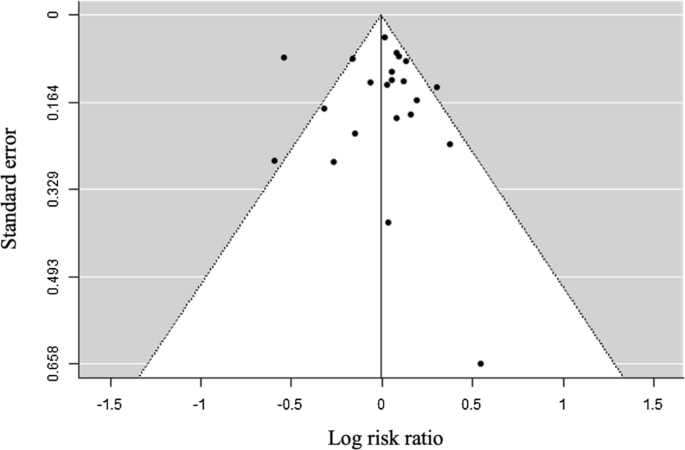
— Publication bias was checked (and excluded) by visual inspection of funnel plots (log risk ratio against standard errors) and a regression test for funnel plot asymmetry. (What is Publication bias? This is when the outcome of a study influences the decision to publish or not. Publishing only results that show a significant finding inserts a “publication bias” in favor of positive results. Checking for the distribution of outcomes across all studies can help identify whether publication bias misinforms the outcome of a meta-analysis.
Funnel plot of the overall differences between injury rate of female and male runners (log risk ratios against standard error).
— The meta-analysis used a random-effects model, which estimates the mean effect in a range of studies and does not cause the overall effect size estimate to be overly influenced by the size of any one study. On the contrary, in a fixed-effects model, we assume that the true effect size for all studies is identical; smaller weights are assigned to smaller studies, and vice versa, which means that a fixed effect model largely ignores information in the smaller studies.
— Between-study heterogeneity was calculated. I.eHow variable were the outcomes between studies? If heterogeneity is large, we have less confidence in the overall effect.
What were the weaknesses?
— The specific injury risks were based on a very small number of studies (5 studies for bone stress injuries and 2 studies for Achilles tendon injuries).
— There was a moderate to high heterogeneity between studies included in the overall injury meta-analyses. Therefore, there is a need for further studies with a clear injury definition and standardised data collection procedures.
— Due to the lack of published studies, this systematic review did not allow conclusions on the sex-dependent epidemiology of pathologies other than bone stress injuries and Achilles tendinopathies.
— Many studies lacked specific info concerning training load (mileage, training duration) and competition distances, limiting the accuracy of conclusions made.
Are the findings useful in application to training/coaching practice?
Yes.
It is important for athletes and coaches to be aware of injury risk. In this meta-analysis, 20% (or 1 in 5) of athletes had at least 1 injury. Appropriate training load management, recovery management (nutrition, sleep, rest), and strength training strategies must be used to help mitigate injury risk. These findings also highlight the importance of stress fracture-related injuries in female runners, which are typically caused by low energy availability induced through a combination of poor training load management and inadequate nutritional needs to support bone turnover (low dietary calcium, iron, and vitamin D). It is also important to note that although such risks are lower in males runners, the risk is lower not zero.
What was the hypothesis or research question?
Because elite athletes have a higher fractional utilisation of VO2max — i.e. they can sustain higher fractions of max for longer — than sub-elite and untrained folks, it is likely that the relationship between relative heart rate (% of max) and oxygen consumption (VO2, % of max) may differ between these groups. Because there is also a lack of info in this area for elite athletes, the authors compared elite endurance athletes’ ratings of perceived exertion (RPE) with heart rate, VO2, and lactate during low to high steady-state exercise intensities. By doing so they hoped to provide an evidence-based framework for developing intensity scales for elite endurance athletes
What did they do to test the hypothesis or answer the research question?
— Pre-existing data from 160 elite male (VO2max ~77 mL/kg/min) and female (VO2max ~64 mL/kg/min) cross-country skiers, biathletes, orienteers, mountain bikers, road cyclists, and speed skaters on the Norwegian national team were retrospectively extracted from a database at the Norweigan Olympic training center.
— Data included submaximal and maximal exercise test data. A running test was used in the cross-country skiers, biathletes, and orienteers, while a cycling test was used in the mountain bikers, road cyclists, and speed skaters.
What did they find?
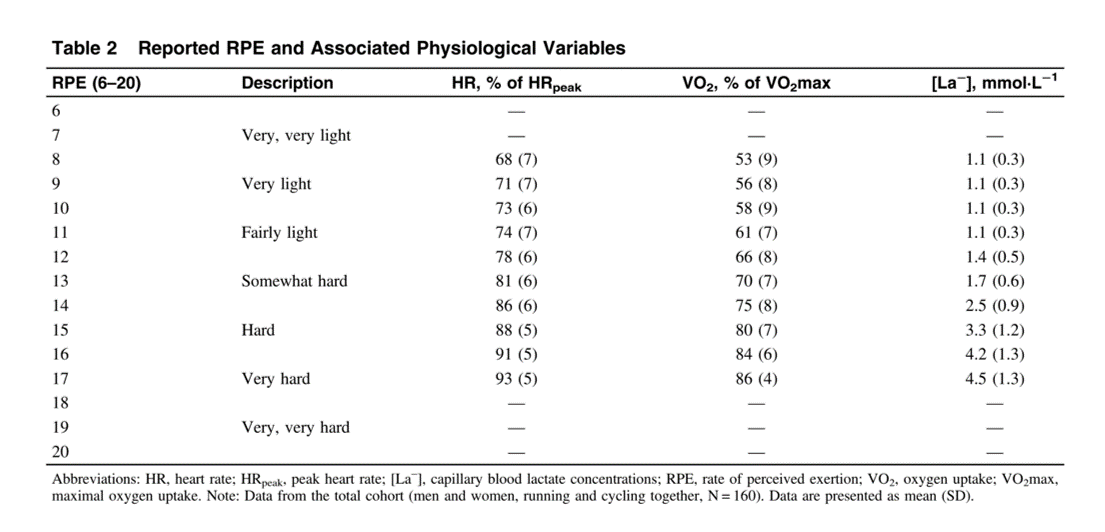
— The following table shows the raw data:
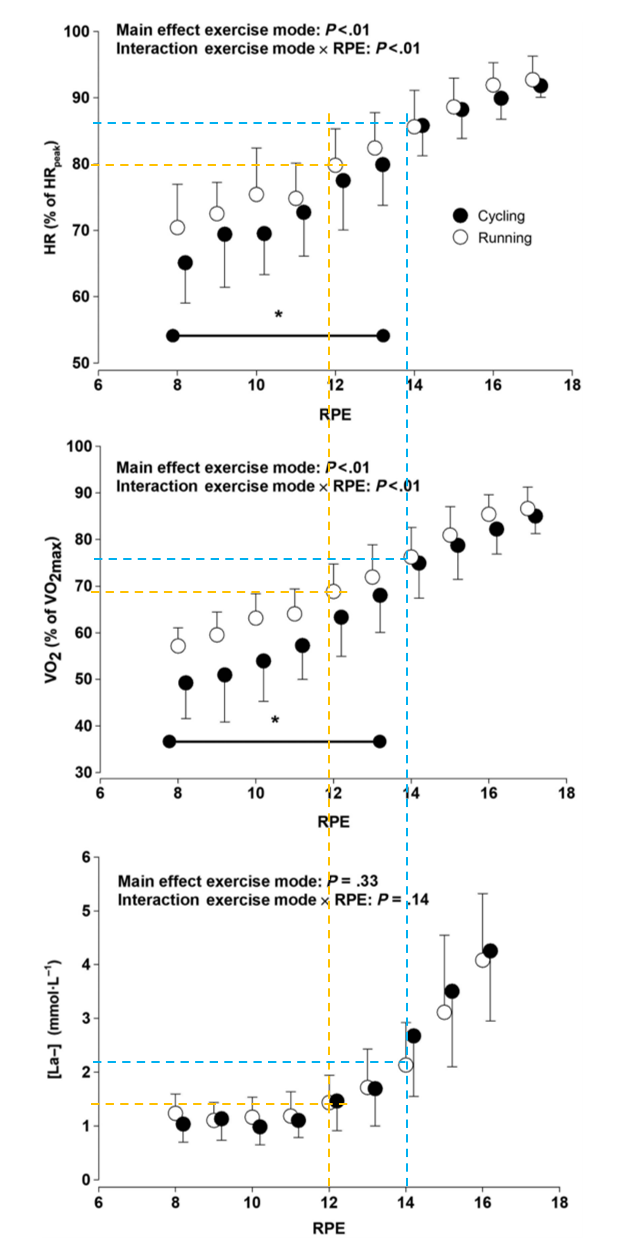
— Regression analyses showed strong relationships between RPE and %HR (r = 0.80, P < .05), RPE and %VO2 (r = 0.82, P < .05), and RPE and lactate (r = 0.80).
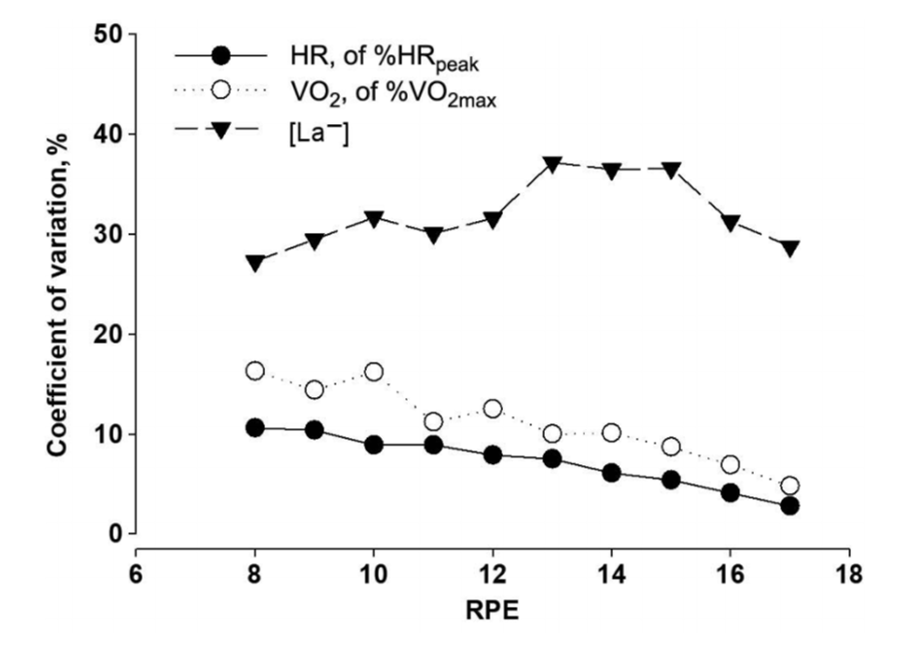
— But there was also large between-subject variation (10% to 30%
coefficient of variationa standardised measure of spread relative to the mean, calculated as the standard deviation divided by the mean value multiplied by 100.
) in %HR, %VO2, and lactate values, especially at lower intensities.
— There were no sex differences in the relationships but the authors’ analyses did reveal an affect of exercise mode on %HR and %VO2 where the heart rate and VO2 values were higher during running than cycling at lower intensities (RPE <14>
The %HR, %VO2, and [La−] as a function of RPE for running and cycling. HR indicates heart rate; %HR, relative heart rate; HRpeak, peak heart rate; [La−], blood lactate concentration; RPE, rate of perceived exertion; VO2, oxygen uptake; %VO2, relative oxygen uptake; VO2max, maximal oxygen uptake. * represents the area of differences between exercise modes (P < 05).
What were the strengths?
— Thorough description of metabolic testing and use of standardised submaximal and maximal tests in all participants.
— Large cohort of elite athletes.
What were the weaknesses?
— The retrospective design means that the subjects were not recruited for the purpose of this study. It is unclear what stage of training athletes were in — off-season lack of fitness vs. race-season peak fitness may influence the relationship being probed in the study.
— The retrospective design also means that different test operators would have run the exercise tests and measured the variables, introducing bias.
— In a study examining inter-individual variability it was a pity that only mean and standard deviations were presented. Box plots showing medians, interquartile ranges and 95% confidence intervals, would be more informative.
— The addition of ventilation data (to assess VO2 per breath, changes in which allow us separate “Easy” from “moderate” from “heavy” domains) and self-reported feelings of breathing rate and talk-test would have allowed for greater practical application.
Are the findings useful in application to training/coaching practice?
Yes.
It is important for athletes and coaches to acknowledge that standard exercise guidelines, devices, and metrics, etc, prescribe and/or monitor intensity using arbitrary “zones”, with specific relative heart rate thresholds. For example, Polar and Garmin’s 5-zone model uses 90%, 80%, 70%, 60%, and 50% of HRmax to delineate zones 5, 4, 3, 2, and 1. They then tell you that zone 1 and 2 are “aerobic”, which means than your “aerobic threshold” falls at the top end of zone 2 at 60% of your HR max, and that zone 5 is “anaerobic”, meaning that your “anaerobic/lactate threshold” falls at the top of zone 4 at 90% of your HRmax. The problem with the fixed relative percentages is that they are a complete guess; the true demarcations that separate the biological intensity domains are massively-variable between people.
Let’s take the recent Breaking2 project as an example — the lactate threshold of athletes selected for Breaking2 ranged from 87% to 97% of VO2max . So, if these athletes trained using the 5-zone model, which tells them that their lactate threshold occurs at 90%, the majority of them would essentially “de-train”. On the contrary, I have conducted exercise tests in older-aged folks with obesity and type 2 diabetes; in some of them, their lactate threshold occurred at about 75-80% of HRmax. Therefore, the 5-zone model would push these folks too hard. The point of the matter is that, if you wish to use intensity zones to polarise your training, intensity zones should always be individualized. Lab testing is required to find your biological intensity domains but this is costly and needs regular re-testing. An alternative is to assess your RPE along with your breathing rate and the talk test, both of which can provide valuable info about which domain you are in… Breathing easy and fully-conversational = Easy domain, less than aerobic threshold. Breathing rapidly but deep and controlled and only able to speak a few words = on the cusp of the Heavy domain at your lactate threshold.
What was the hypothesis or research question?
Depending on where you live, face masks may be required in public places. Several studies have examined the effects of N95 and surgical masks on the cardiovascular and subjective response to exercise but cloth face masks appear to be the most common type of mask used by the general public. Therefore, examining the impact of wearing a cloth face mask on subjective and objective cardiopulmonary response to maximal exercise and performance is needed. Therefore, the authors sought to determine if wearing a cloth face mask significantly affected perceptual measures of effort, exercise performance and associated physiological responses during a maximal treadmill test.
What did they do to test the hypothesis or answer the research question?
— 31 young, healthy, physically-active individuals completed both trials, including 14 women and 17 men, 24 of whom had worn a face mask while exercising prior to the study.
— Participants completed two experimental trials approx 8 days apart in a counterbalanced order. During each trial, they completed a cardiopulmonary exercise test (CPET) following a Bruce treadmill protocol of 3-minute stages at progressively-increasing workloads to volitional fatigue.
— At the end of each stage during the test, RPE and heart rate were recorded, and breath-by-breath indirect calorimetry was used to measure oxygen consumption (VO2), carbon dioxide production (VCO2), respiratory exchange ratio (RER), minute ventilation (VE), breathing reserve (BR), respiratory frequency (RF) and tidal volume (VT). A Scale of Measuring Subjective Perceptions to mask-wearing was also used to assess humidity, heat, breathing resistance, itchiness, tightness, saltiness, feeling unfit, odour and fatigue.
What did they find?
— Wearing a cloth mask reduced total exercise time during the treadmill test, which was used as a marker to show reduced “exercise performance”.
— Wearing a cloth mask also reduced VO2max (32.2±9.0 vs. 43.9±8.1 mL/kg/min; P<0.001, Cohen’s d effect size = 1.51, a very large effect). There were also significant reductions in ventilation rate (huge effect size 2.23), breathing reserve (very large effect size 1.94), respiratory frequency (large effect size 1.09), and tidal volume (large effect size 1.5).
— At VO2max, wearing a mask did not affect maximal heart rate, RPE, blood oxygen saturation, or blood pressure.
— However, at submaximal intensities, the cloth mask increased RPE (moderate effect) and reduced blood oxygen saturation (moderate to large effect).
— Participants also reported feeling increasingly short of breath (dyspnoea) and claustrophobic at higher exercise intensities while wearing a cloth face mask, compared to when not wearing the mask.
— It is possible that the reduction in “exercise performance” (i.e. less total exercise time) was due to subjects’ perceived discomfort associated with mask-wearing.
What were the strengths?
— Randomised controlled trial with a
cross-overAll subjects underwent all trials.
design.
— Power calculations to justify the sample size.
— Included men and women.
— Reporting effect sizes.
What were the weaknesses?
— Since the authors chose not to adjust P values for multiple comparisons (“due to the exploratory nature of this study”) it is possible that type 2 errors are arising in the serial measurements of variables during the exercise test. For example, when heart rate is measured at 5 consecutive time points during a test, each time point is not independent from the other and so we would typically adjust the “significance” criterion threshold of the P-value by the number of serial measurements (in this case, 0.05 would be divided by 5 time points, therefore the “significance” criterion should be P<0.01 not P<0.05).
Are the findings useful in application to training/coaching practice?
Yes.
Increasing evidence suggests that wearing either a cloth, N95, or surgical mask during exercise can decrease VO2 and increase RPE along with increased feelings of anxiety, claustrophobia. Coaches and athletes should be aware of these findings firstly because wearing a mask during exercise is not pleasant but also because trying to train at the same workloads as you would without a mash will cause a greater cardiovascular strain (higher VO2 and higher HR response) along with a greater level of perceived exertion (RPE). Therefore, to prevent excessive training load when wearing a mask, you should reduce your absolute workload to achieve the same relative workload. E.g. if your interval run pace is normally 4 min/km without a mask then you will need to go a little slower with a mask to elicit a similar heart rate, breathing rate, and RPE.
Notably, masks are only mandated indoors in most countries. Few countries have mandated masks for outdoor exercise (i.e. exercise in wide, open, well-ventilated spaces). So, if possible, go train outside. As coaches, Matt and I would always encourage athletes to train on the terrain on which they will race as much as possible — so get your ass outside.
What was the beer called?
Stiegl-Goldbräu.
Which brewery made it?
Stiegl Brauwelt, Salzburg, Austria.
What type of beer is it?
Kölsch-style full beer.
How strong is the beer (ABV)?
5.0 % ABV.
How would I describe this beer?
Smells like the morning after a belly full of lager but is light on the tongue, gently bitter to the taste and refreshing on the way down the hatch with a slightly tangy aftertaste. An ice-cold Stiegl-Goldbräu is a perfect sit-in-the-sun-after-work boozer but it won’t turn you into a superlative-addicted beer geek.
What is my Rating of Perceived beer Enjoyment?
RP(be)E(r) = 6 out of 10.
What was the hypothesis or research question?
A runner's high is a common feeling of euphoria associated with reduced anxiety following exercise. Two potential mechanisms for runners high have been identified, endocannabinoids and opioids. Previous work in mice has shown that opioids are not responsible for runner's high, but this has not been verified in humans. The objective of this study was to validate this findings in humans that opioids are not responsible for the sensation of the runners high.
What did they do to test the hypothesis or answer the research question?
— Researchers performed a double blind, placebo controlled study on 63 individuals (32 in the treatment group, 31 in the placebo). The treatment group received the opioid receptor antagonist NAL and the placebo group received an identical looking placebo pill.
— Each group walked (less than 50% of their age adjusted heart rate max) and ran for 45 minutes (at 70 - 85% of their age adjusted heart rate max) on the treadmill on separate occasions and noted their emotional state using a visual analog scale, the Acrophobia questionnaire, the Spielberger State-Trait Anxiety Inventory, and the Sensation Seeking Scale Form V. Anxiety was also assessed using the a elevated plus-maze in a virtual reality setting.
— Blood endocannabinoids were measured and normalized to hematocrit.
What did they find?
— Running increased the levels of endocannabinoids to a greater degree, had more subjects subjectively report a runners high (about ⅓ of them), increased euphoria (medium to large effect size), and decreased anxiety (small to medium effect size).
—. There was no difference in any of the measures in the group of runners given the opioid blocker NAL.
— Walking also increased endocannabinoids, but to a lesser degree than running did.
What were the strengths?
— Double blinded, placebo controlled.
— Multiple measures of anxiety.
— Walking as a control for each individual.
What were the weaknesses?
— Relatively low number of subjects reported as having experienced a runners high (12 of 62).
— Why not have subjects take the placebo and the opioid inhibitor?
— Lab conditions are unlikely ideal to reproduce the runners high.
Are the findings useful in application to training/coaching practice?
Not really. It’s an interesting study and certainly the runner's high has a lot of value to runners themselves, but this study does nothing to further a way coaches could enhance that experience for athletes. Athletes themselves should recognize that the runner's high is a real physiological phenomenon and use running as a positive stressor on their psyche.
What was the hypothesis or research question?
Many physiological processes have diurnal patterns throughout the day. Ultrarunning events often have both a daytime and nocturnal portion of the race due their length. One potential diurnal physiological process is the neuroendocrine factors associated with gastrointestinal function and exercise-induced gastrointestinal syndrome is common in ultrarunners. As such the researchers hypothesized that given their diurnal patterns that prolonged nocturnal running would increase the incidence and severity of gastrointestinal issues.
What did they do to test the hypothesis or answer the research question?
— 16 runners (n = 8 females) were recruited to conduct 3 hours of exercise at 70% of VO2max either starting at 0900h or 2100h.
— RPE, HR, and gastrointestinal symptoms were recorded every 15 minutes during the exercise and gut transient/mobility was measured starting at 150 minutes of exercise.
— Blood samples were taken prior to and post exercise for blood markers of gastrointestinal distress (sCD14, I-FABP, LBP, and IL-1beta)
What did they find?
— I’m tempted to leave it at this quote “Two participants did not complete the NIGHT trial due to severe symptoms including nausea, pro- jectile vomiting, and explosive bowel movements during exercise. Another participant on NIGHT experienced projectile vomiting immediately postexercise.” But I will expand. Night running was associated with significantly higher upper and lower gastrointestinal symptoms and severity of those symptoms. These were moderate - strong effect size differences.
— The only blood markers of gastrointestinal stress were also elevated at night relative to during the day was cortisol, whereas several of the others increased in response to exercise but did not differ from night to day (I-FABP for example).
— Gastrointestinal transit time was significantly slower during the night versus the day.
What were the strengths?
— Looked at many different aspects of gastrointestinal stress. Subjective, objective blood markers, and even transit time.
— Controlled for diet the day of given a low FODMAP diet and attempted to control for food prior to the 3 hour run.
What were the weaknesses?
— There were differences in the total food consumption immediately prior to the exercise.
— Not necessarily a weakness but the runners were considered recreational in nature and not elite, which may have resulted in a different outcome.
— During exercise the food and drink was not ad libitum for the first 2 hours of running.
Are the findings useful in application to training/coaching practice?
Yes. Gastrointestinal issues make it difficult to hydrate and eat ideally during an ultra, which may compromise performance. Thus, time of day should be considered and diurnal fueling strategies may need to be considered depending on an individual's sensitivity to night time gastrointestinal issues. Training sessions at night may help individuals determine whether such issues might arise and allow for a modified night fueling plan to limit symptoms.
What was the beer called?
La Nina
Which brewery made it?
Lost Grove Brewery collaboration with The Ram, Boise, ID, USA
What type of beer is it?
Helles Bock
How strong is the beer (ABV)?
8.4% ABV.
How would I describe this beer?
Has a sweet bready flavor without much nose. There is a hint of bitterness on the backend from some hops that provides a sharp finish to what tastes more like a high alcoholic pilsner than anything. Although I probably would have been happy with a sweeter finish as well. Solid alternative when you are not in the mood for taste buds getting destroyed.
What is my Rating of Perceived beer Enjoyment?
RP(be)E(r) = 7 out of 10.
That is all for this month's nerd alert. We hope to have succeeded in helping you learn a little more about the developments in the world of running science. If not, we hope you enjoyed a nice beer…
Until next month, stay nerdy and keep training smart.
Everyday is a school day.
Empower yourself to train smart.
Think critically. Be informed. Stay educated.
Disclaimer: We occasionally mention brands and products but it is important to know that we are not sponsored by or receiving advertisement royalties from anyone. We have conducted biomedical research for which we have received research money from publicly-funded national research councils and medical charities, and also from private companies. We have also advised private companies on their product developments. These companies had no control over the research design, data analysis, or publication outcomes of our work. Any recommendations we make are, and always will be, based on our own views and opinions shaped by the evidence available. The information we provide is not medical advice. Before making any changes to your habits of daily living based on any information we provide, always ensure it is safe for you to do so and consult your doctor if you are unsure.
If you find value in these nerd-alerts, please help keep them alive and buy us a beer:
If you enjoy this free content, please like and follow @veohtu, @mjlaye and @thomaspjsolomon and share these posts on your social media pages.
About the authors:
Matt and Thomas are both passionate about making science accessible and helping folks meet their fitness and performance goals. They both have PhDs in exercise science, are widely published, have had their own athletic careers, and are both performance coaches alongside their day jobs. Originally from different sides of the Atlantic, their paths first crossed in Copenhagen in 2010 as research scientists at the Centre for Inflammation and Metabolism at Rigshospitalet (Copenhagen University Hospital). After discussing lots of science, spending many a mile pounding the trails, and frequent micro brew pub drinking sessions, they became firm friends. Thomas even got a "buy one get one free" deal out of the friendship, marrying one of Matt's best friends from home after a chance encounter during a training weekend for the CCC in Schwartzwald. Although they are once again separated by the Atlantic, Matt and Thomas meet up about once a year and have weekly video chats about science, running, and beer. This "nerd alert" was created as an outlet for some of the hundreds of scientific papers they read each month.
To read more about the authors, click the buttons:
 and Matt Laye PhD
and Matt Laye PhD 
 What was the hypothesis or research question?
What was the hypothesis or research question?